Medical Insights
Real Cases Anonymised
Medical Insights — Real or simulated cases inspired by actual maritime and emergency medicine experience.
All cases are anonymised and adapted for educational purposes. No medical advice is intended.
Stroke Managed 300 Nautical Miles from Shore
During a private transatlantic crossing, a senior guest experienced sudden neurological symptoms…
Severe Heat Stroke During Tropical Navigation
A young crew member collapsed on deck during routine maintenance under intense midday sun…
Anxiety and Insomnia During Travelling
A high-profile guest began experiencing worsening anxiety and insomnia during a long crossing…
Rope Injury on Deck: Deep Laceration in a Seafarer
While securing mooring lines, a deckhand sustained a traumatic injury to the forearm…

Stroke Managed 300 Nautical Miles from Shore
Context:
During a private transatlantic crossing aboard a luxury yacht, a senior guest with only medical background of hypertension treated with Enalapril 20mg per day, experienced sudden neurological symptoms, 300 nautical miles from the nearest land.
Situation:
The individual presented with sudden weakness on the right side of the body, slurred speech, and slight confusion — classic warning signs of an acute cerebrovascular accident (stroke). Immediate action was critical, as time-sensitive interventions dramatically influence outcomes.
Medical Action Taken:
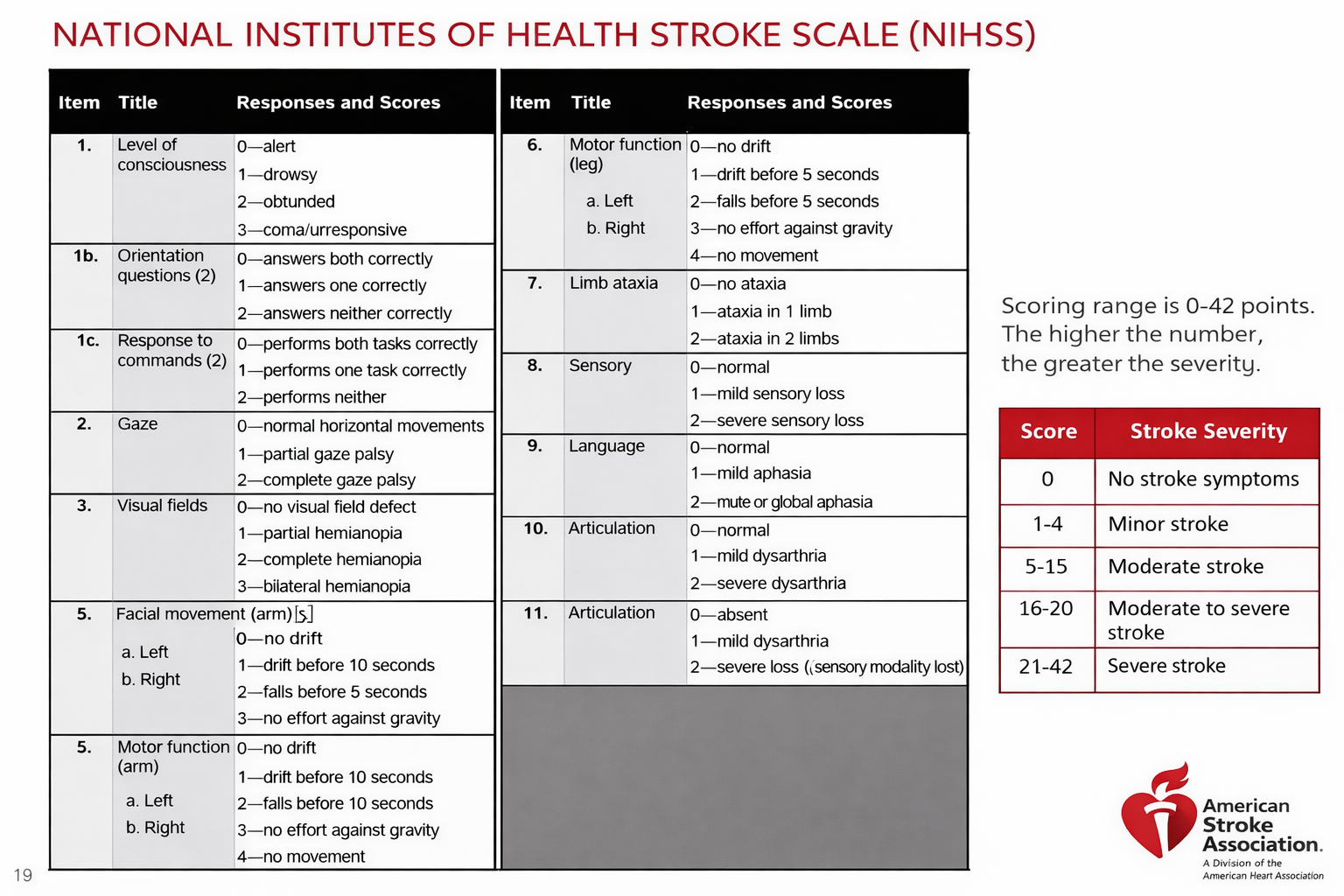
Onboard protocols were activated immediately. A focused neurological evaluation (NIHSS scale) was performed, identifying moderate expressive aphasia and right-sided hemiparesis.
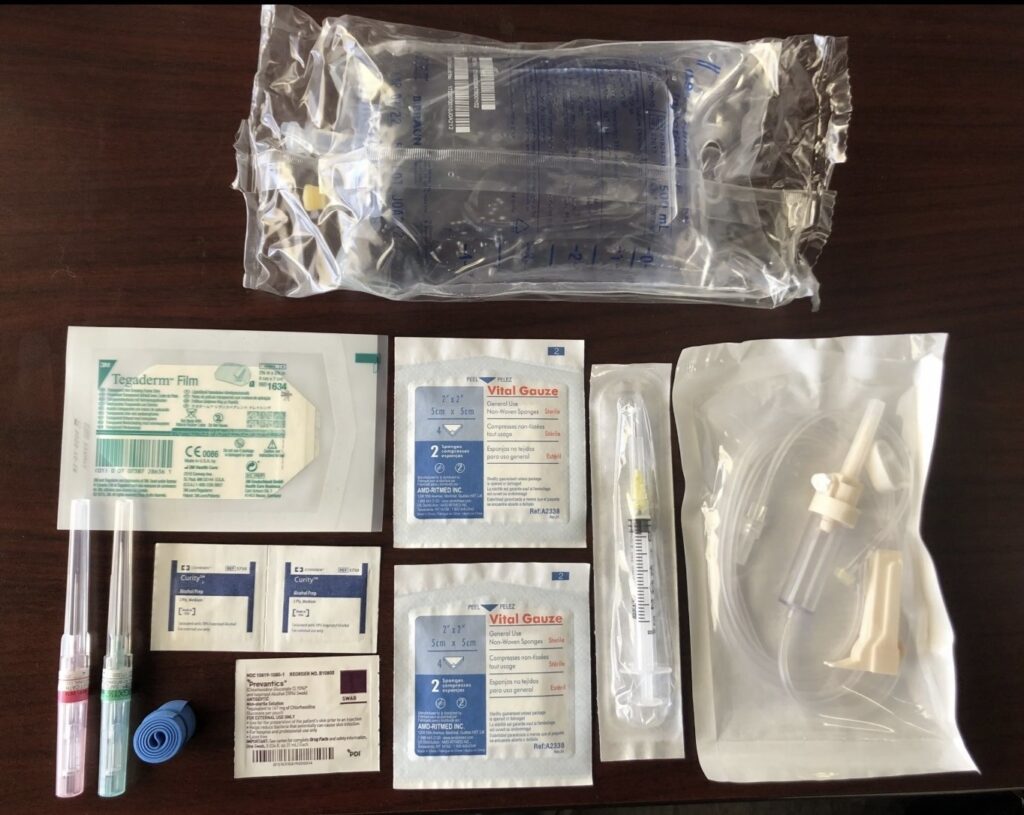
Oxygen was administered at 4 L/min via nasal cannula; blood pressure was carefully managed with Labetalol 10 mg IV (slow bolus) due to systolic pressure exceeding 180 mmHg.
IV hydration with 0.9% saline was started, and core temperature maintained to reduce cerebral demand. Given the timing and distance from definitive care, thrombolysis was excluded, and the goal was rapid stabilization.
A satellite-based teleconsultation was initiated with a land neurologist to assist in monitoring and recommend next steps. Evacuation was coordinated with the yacht’s support team to be executed once within helicopter range (~12 hours later).
Outcome:
The patient remained stable during the next 12 hours and was successfully transferred to a specialized stroke center upon reaching the evacuation zone. Early interventions helped minimize long-term damage.
Insight:
Having a trained medical professional onboard allowed immediate recognition and stabilization, preventing critical delays in a time-sensitive emergency where “every minute saves brain tissue.”

Severe Heat Stroke During Tropical Navigation
Context:
While navigating through equatorial waters during a private charter, a young crew member collapsed on deck during routine maintenance under intense midday sun. As a medical background, he was treating anxiety with daily doses of 40mg of fluoxetine Prozac®
Situation:
The individual was found confused, disoriented, and with dangerously high body temperature exceeding 40°C (104°F). Immediate cooling measures were critical, as heat stroke can rapidly cause multi-organ failure if untreated.
Medical Action Taken:
Diagnosis of classic exertional heat stroke was confirmed: temperature above 40°C, altered mental status, and dehydration signs. It could has been favored by the pro-serotonergic function of fluoxetine.
Immediate core cooling was prioritized: ice packs to axillae, neck, and groin; wet towels and fanning; and chilled IV fluids (500 mL of 0.9% NaCl over 30 min, repeated as needed).
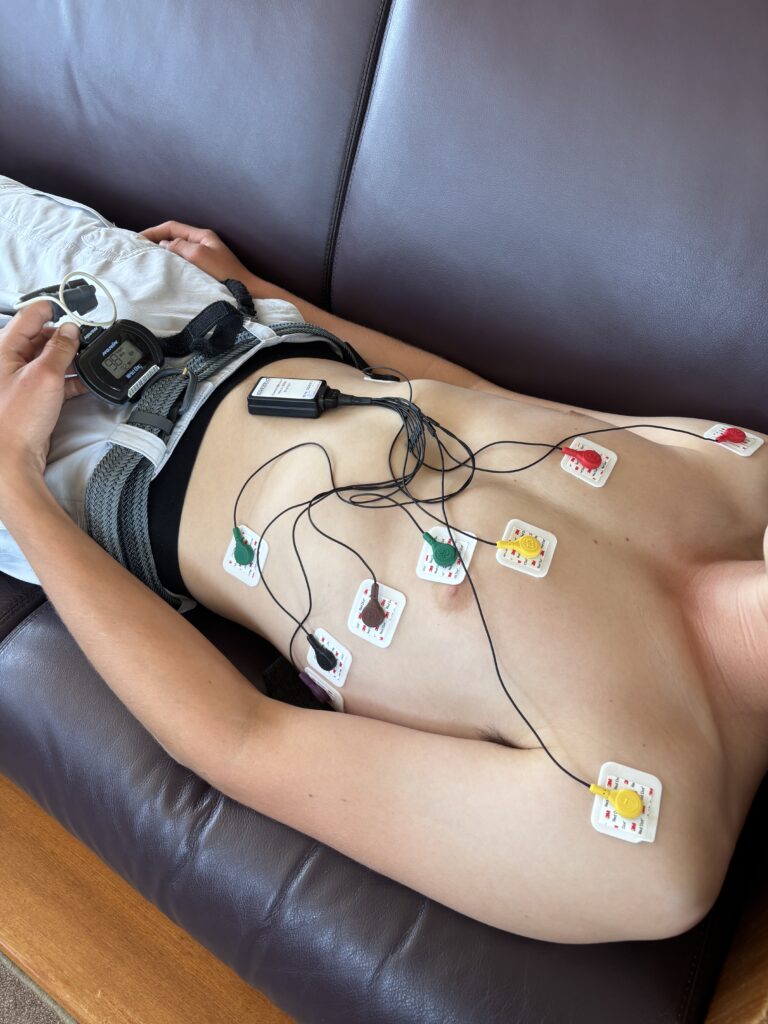
Rectal temperature monitoring was used if available; if not, axillary and tympanic values were closely tracked.
Mild hypotension was managed with fluid resuscitation only; no vasopressors were required.
No antipyretics (paracetamol/NSAIDs) were administered, as they are ineffective in heat stroke and may worsen hepatic stress.
Once stabilized, the patient was given oral rehydration salts (ORS) and kept under observation for 48 hours.
Outcome:
Thanks to early intervention, body temperature was progressively reduced within the critical first hour. The crew member recovered fully with no neurological damage and resumed duties after a monitored rest period.
Insight:
Early recognition and immediate response to environmental emergencies are crucial at sea, where extreme conditions can escalate rapidly. Having a trained physician onboard made the difference between full recovery and potentially fatal complications.

Anxiety and Insomnia During Travelling
Context:
A high-profile guest aboard a Mediterranean-to-Indian Ocean crossing began experiencing worsening anxiety and insomnia after several days at sea, particularly during night navigation and rougher waters.
Situation:
The guest reported intense difficulty falling asleep, early morning awakenings, and escalating restlessness. They described intrusive thoughts, heart palpitations, and physical tension — symptoms consistent with acute anxiety triggered by isolation and disrupted circadian rhythm.
No previous psychiatric diagnosis was known, but they had a long history of work-related stress and occasional use of sleep aids.
Medical Action Taken:
A confidential consultation was conducted in a quiet, private setting to allow the guest to express concerns freely.
Initial assessment ruled out somatic causes (e.g., thyroid, cardiovascular, medication side effects). The patient acknowledged intermittent self-medication with Zolpidem (10 mg) and Alprazolam (0.5 mg) obtained over-the-counter in prior travels — but with poor sleep quality and rising dependency concerns.
A short-term plan was initiated:
Nighttime protocol with low-dose Hydroxyzine (25 mg) for anxiety and sleep, avoiding benzodiazepines onboard unless strictly necessary.
Light dietary and sleep hygiene adjustments (magnesium-rich snacks, screen reduction, controlled ambient lighting).
A progressive muscle relaxation audio program provided privately through the onboard system.
Consideration of Melatonin (2–3 mg) if circadian rhythm disruption persisted.
Daily discreet follow-ups were conducted to adjust dosages and monitor emotional and physical response.
Outcome:
After 72 hours, the guest reported significant improvement: reduced anxiety, increased ability to fall and stay asleep, and improved mood. No sedatives were needed beyond day four. They later thanked the crew discreetly for the calm, “invisible” support and regained full enjoyment of the voyage.
Insight:
Luxury travel may trigger emotional vulnerabilities in even the most successful individuals. A physician onboard provides not only emergency care, but also discreet psychological support that helps guests feel safe, heard, and respected.

Rope Injury on Deck: Deep Laceration in a Seafarer
Context:
While securing mooring lines during a port departure, a deckhand sustained a traumatic injury to the forearm when a tensioned rope slipped under pressure.
Situation:
The incident occurred in rough seas with limited maneuverability, 48 hours from the next port. The patient suffered a deep laceration (~6 cm) to the volar aspect of the forearm, with moderate bleeding, visible subcutaneous tissue, and potential risk to underlying structures. No neurovascular compromise was evident on initial examination, but pain and functional impairment were significant.
Medical Action Taken:
Under sterile conditions, the wound was irrigated thoroughly with 0.9% saline and antiseptic solution (e.g., Povidone-iodine 10%), followed by gentle debridement of devitalized tissue.
After verifying tendon integrity and absence of arterial bleeding, the wound was closed using 3-0 nylon interrupted sutures, and a compression dressing applied.
Prophylactic antibiotic coverage was initiated with Amoxicillin-Clavulanate 875/125 mg every 8 hours for 7 days, given the marine environment and contamination risk.
Analgesia included Dexketoprofen 25 mg three times daily and Paracetamol 1g PRN.
A tetanus booster (Td) was administered due to unknown immunization status.
Wound was monitored daily for signs of infection, and limited-duty instructions were given to protect healing.
Outcome:
Healing progressed without complications, and sutures were removed on day 10 at the next port. The seafarer resumed full duties shortly after.
Insight:
Deck-related injuries, while common, carry high risk of infection and functional impairment if not treated promptly and correctly. Onboard access to advanced wound care supplies and proper antibiotic use ensures crew safety, vessel continuity, and avoids costly port diversions.